

A recent study has shown that symptom relief for treatment-resistant depression (TRD) occurs faster with the use of the IV form of ketamine than with nasal Esketamine (Spravato). TRD is a subset of major depressive disorder where patients do not respond to traditional and first-line therapeutic options. More specifically, TRD is defined as an inadequate response to at least two trials of antidepressants. At Innerbloom Ketamine Therapy, we often encounter patients who have tried multiple antidepressants, unfortunately experiencing little relief from their depressive symptoms, or worse yet, no relief at all. Additionally, it is not uncommon for patients to experience multiple side effects from these medications, which makes the whole situation somewhat confusing. Deciphering which medications are effective can be incredibly difficult. Additional medications are sometimes started solely to combat the side effects of another. Today, we will discuss TRD, compare the two forms of ketamine, review the science and history of ketamine for the treatment of depression, and explain why, at Innerbloom Ketamine Therapy, we offer IV ketamine instead of nasal Esketamine for TRD.
For a succinct review of the top studies regarding the utilization of ketamine therapy for depression treatment, I encourage you to read our blog post titled "Ketamine Therapy for Depression Treatment: Key Scientific Studies Over the Past Two Decades (Updated 2024)."

Major depressive disorder (MDD) is very common, affecting 1 in 10 Americans. Depression is a risk factor and linked to several health conditions, including diabetes, cancer, heart disease, lupus, multiple sclerosis, arthritis, Parkinson’s disease, and more. The American Heart Association lists depression as the fourth major risk factor for coronary heart disease, alongside other factors, such as smoking, hypertension, diabetes, and hyperlipidemia. People with depression are more likely to have a cardiovascular event such a heart attack or stroke. Treatment for MDD using traditional antidepressants can be ineffective, with only 30% being able to achieve full recovery or remission. The remaining 70% of patients suffering from MDD will either respond without remission (20%) or not respond at all (50%). According to the Mayo Clinic, “almost a third of the nearly 9 million people in the United States treated for depression each year have TRD. Given how common TRD may be, limitations in medication options — typically a crucial component of depression treatment plans — are a significant roadblock”.
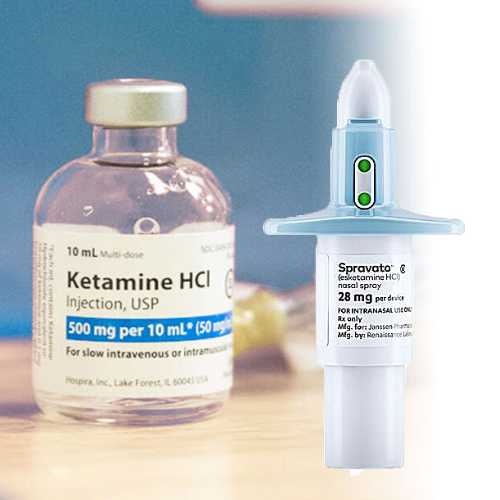
Esketamine is the nasal form of ketamine administered at doses of 56 or 84 mg. However, the bioavailability of nasal Esketamine is approximately 40%. The actual dose received may be inconsistent as it depends of factors such as the absorption of the medication in the nose and other parts of the aerodigestive tract. Bioavailability refers to the rate and extent to which a drug is absorbed and reaches circulation. IV Ketamine is 100% bioavailable, which means that IV doses are much less than other forms of ketamine, but deliver more potency than the other forms with lower bioavailability. Additionally, IV ketamine allows for precision. This is beneficial for subsequent infusions, because doses are incrementally increased to improve efficacy and to find the dose with the most therapeutic potential for each patient. To do this is challenging for nasal and oral forms of ketamine, as the actual received dose can be somewhat of a guessing game. The added benefit of IV ketamine is that if a patient develops nausea or other side effects, they can be easily treated immediately because the patient is being closely monitored and has IV access. Additionally, an infusion can be stopped at any time, which is not the case for the nasal from of ketamine.
Ketamine is not a new medicine. It was first synthesized in 1962 by Calvin Stevens as an analog for PCP. Although PCP has a bad reputation, it was a very effective anesthetic. The problem with PCP, however, was that when patients came out of anesthesia, they sometimes experienced ‘emergence reactions’, with symptoms including hallucinations, convulsions, and aggression that mirrored schizophrenia. The PCP molecule was then modified to form ketamine, which did not have any of these undesired side effects. Ketamine was first tested on prisoners in 1964, and was found to be a very effective anesthetic. Observers also noted that when the subjects came out of anesthesia, they experienced improvements in their mood and had less depressive symptoms. Ketamine was FDA approved for general anesthesia in 1970. It was commonly used in the battlefield, especially during the Vietnam war, and is still very commonly used in both the operating room and in emergency situations today.
Ketamine was FDA approved in 2019 for treatment resistant depression in conjunction with an oral antidepressant, then the following year, it was approved for major depressive disorder with acute suicidal ideation or behavior.
IV Ketamine is a mixture of the two isomers, (R)-ketamine and (S)-ketamine. Esketamine contains just the (S)-Ketamine isomer. Previous data indicated that the (S)-ketamine isomer is a more potent anesthetic than (R)-ketamine. However, recent studies suggest more "negatively experienced" psychopathology with (S)-ketamine alone, rather than those receiving IV ketamine which again is mixture of (R/S)-ketamine, Additionally, other studies suggest that the (R)-ketamine may have more antidepressant effects, which means both isomer are important and that IV ketamine is superior to (S)-ketamine alone.
In a recent observational study by Singh et al., they compared the efficacy and interval until remission or response with repeated IV ketamine and Esketamine treatment in adults diagnosed with TRD. Their study included 62 individuals who received up to six IV ketamine infusions (0.5 mg/kg over 40 minutes) or up to eight intranasal Esketamine treatments two to three times per week.
“Results showed that the number of treatments required to achieve both response (two vs. four) and remission (two vs. seven) was significantly lower among those in the IV ketamine group compared with intranasal Esketamine”. Additionally, when adjusting for age, sex, BMI, and baseline depression scores, they found faster responses ,as well as a faster time to remission for IV ketamine.
Today we briefly reviewed findings from a new study that suggests IV ketamine is superior to nasal Esketamine for treatment-resistant depression. We compared IV ketamine to Esketamine, discussed the history and science of ketamine, and lastly explained why at Innerbloom Ketamine Therapy we choose IV over other forms of ketamine, including the nasal spray Esketamine.
Disclaimer: All content on this website, including (but not limited to) this statement, news, blog post, article, testimonial, or FAQ is not medical advice and should not be considered as such. This website cannot diagnose or treat any medical condition. Only a licensed medical professional who is familiar with you and your medical history can do that. Therefore, we cannot be responsible or liable for any actions taken by those who access our website or rely on its content. Please refer to the Terms & Conditions for more information.